
| IB Psychology students spot study then cross their fingers and hope, pray to interventionist gods, bribe teachers ($10,000 minimum, please!), and so on and such forth. Every IB Psychology student has been through this, every IB Psychology teacher has tried to stop his or her students going through this. Picture this, it’s the day of the first IB Psychology topic test of the year – the Cognitive Level of Analysis. Being a nice, kind IB Psychology teacher I have prepared a topic test which, very generously, allows the student a choice of answering one of three short answer questions (SAQs, 8 mark questions) and similarly, one of three extended response questions (ERQs, 22 mark questions). In the IB Psychology examination, there is no choice in the Paper 1 examination. Students file anxiously into the room, there is nervous chatter as they take their seats. I call for silence and distribute the test papers face down. I provide instructions and initiate the start of the test with my usual call to action … “Let’s rock and roll!”. What follows next is a very hard lesson to learn, but it is so much better to learn it at the start of the IB Psychology course, than in the mocks (where predicted grades are often confirmed) or even worse, the final examination. Every single IB student is time poor, there are competing demands from other subjects, TOK, extended essays, CAS requirements, sports, clubs and, of course, friends and just a little bit of a social life. Revision time always has an opportunity cost. I scan faces as my students turn their test papers over, in beautiful synchrony approximately one third of the class will raise their eyes skyward with a thankful little smile on their faces, another third will scrunch their eyes together and silently moan (perhaps a bolder one will bang her head on the desk – “Shhhh, silence!”), another third will take a deep breath, pause and dive in. One group has had their questions turn up, the other group hasn’t and the third group have studied all questions, but not memorised model answers. I could stop them right here, save | 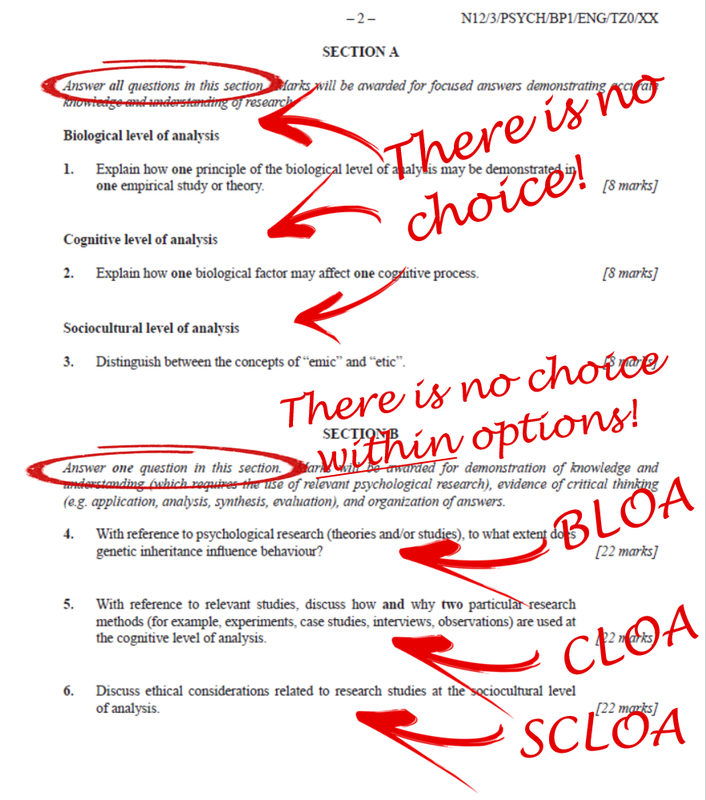 There is no choice in IB Psychology examinations us all a lot of pain. The first group are the 7s, the second group will be very lucky to get 2s, and the third group are my 4s and 5s. Most IB Psychology students spot study. The good ones will learn the lesson early, the not-so-good ones will continue to ride their luck or hope their luck will finally turn. They all know the questions that will be asked (there are no surprises in the IB Psychology exams, see previous post) and will learn and memorise model answers to as many of these as they have time for. Your exams are upon you. Learn all of the model answers to one level of analysis (e.g., BLOA) in the Paper 1 exam and skip two at a maximum for each Paper 2 option (e.g., Abnormal and Human Relationships). Don’t be tempted to ride your luck or hope your luck will change – if the question you haven’t fully prepared for doesn't come up, you will completely wreck two years of hard (and interesting!) work … and, by the way, break your poor IB Psychology’s teacher’s heart in the process. Best of luck for your IB Psychology exams (although we all know we make our own luck). |
Author: Derek Burton – Passionate about IB Psychology
 |  |
Remember, we've taken the hard work out of your IB Psychology exams by preparing complete sets of model answers across both Paper 1 and Paper 2 exams.
















 RSS Feed
RSS Feed