Another ERQ model answer from IB Psychology

Abnormal psychology is based upon the assumption that we know what 'abnormal' is, which in turn, is based upon us knowing what 'normal' is. So, how exactly do we make these judgments?
You're hanging out a LOT in your dark, smelly and incredibly messy bedroom, not talking to family and only interacting with your friends online. Teachers are concerned about you, your family is worried sick. Do you have some sort of social anxiety disorder? Surely this is a manifestation of a mental illness? ... but hang on! Isn't this just 'normal' teenage behaviour?
Have you ever wondered just how easily you could be confined to a mental hospital if say, your parents, didn't like the way you were behaving? If their concepts of normality and abnormality differed from yours? The answer is, probably pretty easily, but not as easily as in the past, and more easily in some countries than in others. Thus, we need some some sort of objective definition or classification of what abnormal behaviour actually is, and how we can make a judgement as to whether someone has a mental illness or not.
The IB Psychology learning outcome: Examine concepts of normality and abnormality, takes a very good look at this thought-provoking issue.
Much of what we examine in the model ERQ answer focuses on Rosenhan's seminal research. Rosenhan (1973) performed some ground-breaking research with his quasi-experimental study. Here, he and his fellow researchers managed to gain admittance to a variety of psychiatric hospitals around the US after presenting themselves and claiming that a voice in their head was saying "empty", "hollow" and "thud". They found that getting committed was very easy, and getting out was very, very hard ...
You're hanging out a LOT in your dark, smelly and incredibly messy bedroom, not talking to family and only interacting with your friends online. Teachers are concerned about you, your family is worried sick. Do you have some sort of social anxiety disorder? Surely this is a manifestation of a mental illness? ... but hang on! Isn't this just 'normal' teenage behaviour?
Have you ever wondered just how easily you could be confined to a mental hospital if say, your parents, didn't like the way you were behaving? If their concepts of normality and abnormality differed from yours? The answer is, probably pretty easily, but not as easily as in the past, and more easily in some countries than in others. Thus, we need some some sort of objective definition or classification of what abnormal behaviour actually is, and how we can make a judgement as to whether someone has a mental illness or not.
The IB Psychology learning outcome: Examine concepts of normality and abnormality, takes a very good look at this thought-provoking issue.
Much of what we examine in the model ERQ answer focuses on Rosenhan's seminal research. Rosenhan (1973) performed some ground-breaking research with his quasi-experimental study. Here, he and his fellow researchers managed to gain admittance to a variety of psychiatric hospitals around the US after presenting themselves and claiming that a voice in their head was saying "empty", "hollow" and "thud". They found that getting committed was very easy, and getting out was very, very hard ...
short videos examining concepts of mental illness and abnormality
| | |
 Just Give Me the Answers! provides you with the complete collection of model answers for all extended response questions in the Paper 1 and 2 IB Psychology exams. This will save you hundreds of hours of work! | Rosenhan's 1973 original article This article, published in the very prestigious 'Science' journal caused a great deal of controversy and forced the Psychiatric industry to examine their understand of, and practices and procedures around the 'mentally ill'. It changed the way we diagnose and assess degrees of mental illness. |
Examine concepts of normality and abnormality
Another exemplar model ERQ answer for the IB Psychology course. This one is from the Abnormal option and if the student manages to replicate in their IB Psychology exams they are guaranteed to be awarded the full possible 22/22 marks.

Examine concepts of normality and abnormality
The presence of a mental disorder may be considered a deviation from mental health norms and hence the study of mental disorders is often known as abnormal psychology. ‘Normal’ and ‘abnormal’, as applied to human behaviour, are relative terms. Many people use these classifications subjectively and carelessly, often in a judgmental manner, to suggest good or bad behaviour. As defined in the dictionary, their accurate use would seem easy enough: ‘normal’ – conforming to a typical pattern and ‘abnormal’ – deviating from a norm. The trouble lies in the word norm. Whose norm? For what age person? At what period of history? In which culture?
The definition of the word abnormal is simple enough but applying this to psychology poses a complex problem. The concept of abnormality is imprecise and difficult to define. Examples of abnormality can take many different forms and involve different features, so that, what at first sight seem quite reasonable definitions, turns out to be quite problematical. There are several different ways in which it is possible to define ‘abnormal’ as opposed to our ideas of what is ‘normal’
Defining normality
Mental health model of normality (Jahoda, 1958)
The model suggests criteria for what might constitute normal psychological health (in contrast to abnormal psychological health). Deviation from these criteria would mean that the health of an individual is ‘abnormal’:
Evaluation of the mental health model of normality
The majority of people would be categorised as ‘abnormal’ if the criteria were applied to them. It is relatively easy to establish criteria for what constitutes ‘physical health’ but it is impossible to establish and agree on what constitutes ‘psychological health’. According to Szasz (1962) psychological normality and abnormality are culturally defined concepts, which are not based on objective criteria.
Taylor & Brown (1988) argue that the view that a psychologically healthy person is one that maintains close contact with reality is not in line with research findings. People generally have positive ‘illusions’ about themselves and they rate themselves more positively than others (Lewinshohn et al., 1980). For example most people rate themselves as being above average in driving ability, and above average in physical appearance, both of which are a statistical nonsense when considering the essential nature of an average.
Further, the criteria in the model are culturally biased value judgements; i.e., they reflect an idealised perception of what it means to be human in a Western culture. For example, self-actualisation (Maslow, 1968) means the achievement of one's full potential through creativity, independence, spontaneity, and a grasp of the real world. The concept of self-actualisation to a South Sudanese in the middle of sectarian strife, war and famine would be nonsensical at that point in time.
Defining abnormality
The mental illness criterion (the medical model)
The mental illness criterion sees psychological disorders (abnormality) as psychopathology. Pathology means ‘illness’ so it literally means ‘illness in the psyche’. The criterion is linked to psychiatry, which is a branch of medicine, specifically, a branch of medicine that deals with the diagnosis, treatment, and prevention of mental and emotional disorders. Patients with psychological problems are seen as ‘ill’ in the same way as those who suffer from physiological illnesses.
Diagnosis of mental illness is based on the clinician’s (clinical psychologist, psychiatrist) observations, the patient’s self-reports and diagnostic manuals (classification systems) that classify symptoms of specific disorders to help doctors find a correct diagnosis. The most widely used classification system is the new DSM-5, which is the fifth edition of the American Psychiatric Association's (APA) Diagnostic and Statistical Manual of Mental Disorders. In the United States the DSM serves as a universal authority for the diagnosis of psychiatric disorders. Treatment recommendations, as well as payment by health care providers, are often determined by DSM classifications.
Being diagnosed or labelled as being abnormal – mentally ill can have striking consequences in this model, as a controversial study designed to test the medical model and its conception of normality and abnormality.
Rosenhahn (1973) – on being sane in insane places
Aim: To test reliability and validity of diagnosis in a natural setting. Rosenhahn wanted to see if psychiatrists could distinguish between ‘abnormal’ and ‘normal’ behaviour.
Procedure: This was a covert participant observation with eight participants consisting of five men and three women (including Rosenhahn himself). Their task was to follow the same instructions and present themselves at 12 psychiatric hospitals in the US. These pseudo-patients telephoned the hospital for an appointment, and arrived at the admissions office complaining that they had been hearing voices. They said the voice, which was unfamiliar and the same sex as themselves, was often unclear but it said “empty”, “hollow”, “thud”.
After they had been admitted to the psychiatric ward, the pseudo patients stopped simulating any symptoms of abnormality. The pseudo patients took part in ward activities, speaking to patients and staff as they might ordinarily. When asked how they were feeling by staff they said they were fine and no longer experienced symptoms. Each pseudo patient had been told they would have to get out by their own devices by convincing staff they were sane.
Results and conclusion: All participants were admitted to various psychiatric wards and all but one were diagnosed with schizophrenia (the other diagnosis was for manic depression). All pseudo-patients behaved normally while they were hospitalised because they were told they would only get out if the staff perceived them to be well enough.
The pseudo-patients took notes when they were hospitalised but this was interpreted as a symptom of their illness by the staff. It took between 7 and 52 days before the participants were released. They came out with a diagnosis (schizophrenia in remission) so they were ‘labelled’.
A follow-up study was done later where the staff at a specific psychiatric hospital were told that imposters would present themselves at the hospital and that they should try to rate each patient whether he or she was an imposter. Of the 193 patients, 41 were clearly identified as impostors by at least one member of the staff, 23 were suspected to be impostors by one psychiatrist, and 19 were suspected by one psychiatrist and one staff member. There were no impostors.
Rosenhahn claims that the study demonstrates that psychiatrists cannot reliably tell the difference between people who are sane and those who are insane. The main experiment illustrated a failure to detect sanity, and the secondary study demonstrated a failure to detect insanity. Rosenhahn explains that psychiatric labels tend to stick in a way that medical labels do not and that everything a patient does is interpreted in accordance with the diagnostic label once it has been applied.
Evaluation: This controversial study was conducted nearly 40 years ago but it had an enormous impact on psychiatry. It sparked off a discussion and revision of diagnostic procedures as well as discussion of the consequences of diagnosis for patients. The development of diagnostic manuals (e.g., DSM-V) has increased the validity and reliability of diagnosis of what is abnormal or normal in terms of mental health, although diagnostic tools are not without flaws.
The method used raises ethical issues (the staff were not told about the research) but it was justified since the results provided evidence of problems in the diagnosis of mental illness (i.e., being non-beneficially abnormal) which could benefit others. There were serious ethical issues with the follow-up study since the staff thought that imposters would present, but they were real patients and may not have had the treatment they needed.
Evaluation of the mental illness criterion
Proponents of the mental illness criterion argue that it is an advantage to be diagnosed as ‘sick’ because it shows that people are not responsible for their acts. For example, an individual who does not get out of bed because they have been diagnosed for depression; i.e., labelled as being ‘depressed’ and not because they are fatigued (a symptom).
Although the origin of some mental disorders (e.g., Alzheimer’s disease) can be linked to physiological changes in the brain, most psychological disorders cannot. Also, critics of the mental illness criterion argue that there is a stigma (i.e., a mark of infamy or disgrace) associated with mental illness.
Abnormality as statistical deviation from the norm
Deviance in this criterion is related to the statistical average. The definition implies that statistically common behaviour can be classified as ‘normal’. Behaviour that is deviant from the norm is consequently ‘abnormal’. In the normal distribution curve most behaviour falls in the middle. A normal distribution curve is a theoretical frequency distribution for a set of variable data (e.g., scores on an IQ test), usually represented by a bell-shaped curve symmetrical about the mean.
The presence of a mental disorder may be considered a deviation from mental health norms and hence the study of mental disorders is often known as abnormal psychology. ‘Normal’ and ‘abnormal’, as applied to human behaviour, are relative terms. Many people use these classifications subjectively and carelessly, often in a judgmental manner, to suggest good or bad behaviour. As defined in the dictionary, their accurate use would seem easy enough: ‘normal’ – conforming to a typical pattern and ‘abnormal’ – deviating from a norm. The trouble lies in the word norm. Whose norm? For what age person? At what period of history? In which culture?
The definition of the word abnormal is simple enough but applying this to psychology poses a complex problem. The concept of abnormality is imprecise and difficult to define. Examples of abnormality can take many different forms and involve different features, so that, what at first sight seem quite reasonable definitions, turns out to be quite problematical. There are several different ways in which it is possible to define ‘abnormal’ as opposed to our ideas of what is ‘normal’
Defining normality
Mental health model of normality (Jahoda, 1958)
The model suggests criteria for what might constitute normal psychological health (in contrast to abnormal psychological health). Deviation from these criteria would mean that the health of an individual is ‘abnormal’:
- The absence of mental illness
- Realistic self-perception and contact with reality
- A strong sense of identity and positive self-esteem
- Autonomy and independence
- Ability to maintain healthy interpersonal relationships (e.g., capacity to love)
- Ability to cope with stressful situations
- Capacity for personal growth and self-actualisation
Evaluation of the mental health model of normality
The majority of people would be categorised as ‘abnormal’ if the criteria were applied to them. It is relatively easy to establish criteria for what constitutes ‘physical health’ but it is impossible to establish and agree on what constitutes ‘psychological health’. According to Szasz (1962) psychological normality and abnormality are culturally defined concepts, which are not based on objective criteria.
Taylor & Brown (1988) argue that the view that a psychologically healthy person is one that maintains close contact with reality is not in line with research findings. People generally have positive ‘illusions’ about themselves and they rate themselves more positively than others (Lewinshohn et al., 1980). For example most people rate themselves as being above average in driving ability, and above average in physical appearance, both of which are a statistical nonsense when considering the essential nature of an average.
Further, the criteria in the model are culturally biased value judgements; i.e., they reflect an idealised perception of what it means to be human in a Western culture. For example, self-actualisation (Maslow, 1968) means the achievement of one's full potential through creativity, independence, spontaneity, and a grasp of the real world. The concept of self-actualisation to a South Sudanese in the middle of sectarian strife, war and famine would be nonsensical at that point in time.
Defining abnormality
The mental illness criterion (the medical model)
The mental illness criterion sees psychological disorders (abnormality) as psychopathology. Pathology means ‘illness’ so it literally means ‘illness in the psyche’. The criterion is linked to psychiatry, which is a branch of medicine, specifically, a branch of medicine that deals with the diagnosis, treatment, and prevention of mental and emotional disorders. Patients with psychological problems are seen as ‘ill’ in the same way as those who suffer from physiological illnesses.
Diagnosis of mental illness is based on the clinician’s (clinical psychologist, psychiatrist) observations, the patient’s self-reports and diagnostic manuals (classification systems) that classify symptoms of specific disorders to help doctors find a correct diagnosis. The most widely used classification system is the new DSM-5, which is the fifth edition of the American Psychiatric Association's (APA) Diagnostic and Statistical Manual of Mental Disorders. In the United States the DSM serves as a universal authority for the diagnosis of psychiatric disorders. Treatment recommendations, as well as payment by health care providers, are often determined by DSM classifications.
Being diagnosed or labelled as being abnormal – mentally ill can have striking consequences in this model, as a controversial study designed to test the medical model and its conception of normality and abnormality.
Rosenhahn (1973) – on being sane in insane places
Aim: To test reliability and validity of diagnosis in a natural setting. Rosenhahn wanted to see if psychiatrists could distinguish between ‘abnormal’ and ‘normal’ behaviour.
Procedure: This was a covert participant observation with eight participants consisting of five men and three women (including Rosenhahn himself). Their task was to follow the same instructions and present themselves at 12 psychiatric hospitals in the US. These pseudo-patients telephoned the hospital for an appointment, and arrived at the admissions office complaining that they had been hearing voices. They said the voice, which was unfamiliar and the same sex as themselves, was often unclear but it said “empty”, “hollow”, “thud”.
After they had been admitted to the psychiatric ward, the pseudo patients stopped simulating any symptoms of abnormality. The pseudo patients took part in ward activities, speaking to patients and staff as they might ordinarily. When asked how they were feeling by staff they said they were fine and no longer experienced symptoms. Each pseudo patient had been told they would have to get out by their own devices by convincing staff they were sane.
Results and conclusion: All participants were admitted to various psychiatric wards and all but one were diagnosed with schizophrenia (the other diagnosis was for manic depression). All pseudo-patients behaved normally while they were hospitalised because they were told they would only get out if the staff perceived them to be well enough.
The pseudo-patients took notes when they were hospitalised but this was interpreted as a symptom of their illness by the staff. It took between 7 and 52 days before the participants were released. They came out with a diagnosis (schizophrenia in remission) so they were ‘labelled’.
A follow-up study was done later where the staff at a specific psychiatric hospital were told that imposters would present themselves at the hospital and that they should try to rate each patient whether he or she was an imposter. Of the 193 patients, 41 were clearly identified as impostors by at least one member of the staff, 23 were suspected to be impostors by one psychiatrist, and 19 were suspected by one psychiatrist and one staff member. There were no impostors.
Rosenhahn claims that the study demonstrates that psychiatrists cannot reliably tell the difference between people who are sane and those who are insane. The main experiment illustrated a failure to detect sanity, and the secondary study demonstrated a failure to detect insanity. Rosenhahn explains that psychiatric labels tend to stick in a way that medical labels do not and that everything a patient does is interpreted in accordance with the diagnostic label once it has been applied.
Evaluation: This controversial study was conducted nearly 40 years ago but it had an enormous impact on psychiatry. It sparked off a discussion and revision of diagnostic procedures as well as discussion of the consequences of diagnosis for patients. The development of diagnostic manuals (e.g., DSM-V) has increased the validity and reliability of diagnosis of what is abnormal or normal in terms of mental health, although diagnostic tools are not without flaws.
The method used raises ethical issues (the staff were not told about the research) but it was justified since the results provided evidence of problems in the diagnosis of mental illness (i.e., being non-beneficially abnormal) which could benefit others. There were serious ethical issues with the follow-up study since the staff thought that imposters would present, but they were real patients and may not have had the treatment they needed.
Evaluation of the mental illness criterion
Proponents of the mental illness criterion argue that it is an advantage to be diagnosed as ‘sick’ because it shows that people are not responsible for their acts. For example, an individual who does not get out of bed because they have been diagnosed for depression; i.e., labelled as being ‘depressed’ and not because they are fatigued (a symptom).
Although the origin of some mental disorders (e.g., Alzheimer’s disease) can be linked to physiological changes in the brain, most psychological disorders cannot. Also, critics of the mental illness criterion argue that there is a stigma (i.e., a mark of infamy or disgrace) associated with mental illness.
Abnormality as statistical deviation from the norm
Deviance in this criterion is related to the statistical average. The definition implies that statistically common behaviour can be classified as ‘normal’. Behaviour that is deviant from the norm is consequently ‘abnormal’. In the normal distribution curve most behaviour falls in the middle. A normal distribution curve is a theoretical frequency distribution for a set of variable data (e.g., scores on an IQ test), usually represented by a bell-shaped curve symmetrical about the mean.
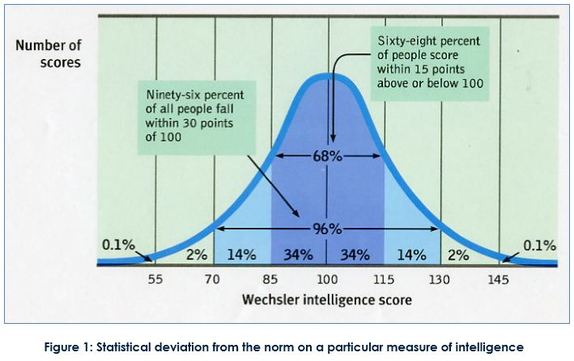
An individual with an intelligence quotient (IQ) of 150 is a deviation from the norm of 100. It is statistically rare but it is considered desirable to have high intelligence. Mental retardation seen as an abnormality in the other direction (sometimes defined as having an IQ below 70) but this is considered undesirable. Obesity is becoming statistically ‘normal’ but obesity is considered undesirable.
Evaluation of the statistical criterion
The use of statistical frequency and deviation from the statistical norm is not a reliable criterion to define abnormal behaviour since what is ‘abnormal’ in a statistical sense may both be desirable and undesirable. What may be considered abnormal behaviour can differ from one culture to another so it is therefore impossible to establish universal standards for statistical abnormality. The model of statistical deviation from the norm always relates to a specific culture.
Abnormality as deviation from social norms
Social norms constitute informal or formal rules of how individuals are expected to behave. Deviant behaviour is behaviour that is considered undesirable or anti-social by the majority of people in a given society. Individuals who break rules of conduct or do not behave like the majority are defined as ‘abnormal’ according to this criterion.
Social, cultural and historical factors may play a role in what is seen as ‘normal’ or ‘abnormal’ within a certain society. For example, around the 1900s in the UK, homosexuality was seen as abnormal and people could be imprisoned or forcibly treated for this ‘mental illness’. Homosexuality was classified as an abnormal sexual deviation in the DSM-II (1968). In later revisions of the manual, homosexuality in itself was not seen as abnormal – only feeling distressed about it was.
Evaluation of the deviation from statistical norms criterion
This criterion is not objective or stable since it is related to socially based definitions that change across time and culture. Further, because the norm is based on morals and attitudes it is vulnerable to abuse. For example, political dissidents could be considered ‘abnormal’ and sent to hospitals for treatment, which was something that occurred in the former Soviet Union. Using this criterion could lead to discrimination against minorities, including people who suffer from psychological disorders.
Psychological disorders may be defined and diagnosed in different ways across cultures and what seems to be a psychological disorder in one culture may not be seen the same way in another culture. The DSM includes disorders called ‘culture-bound syndromes’; for example, penis panic (!) or Koro. This indicates that it is impossible to set universal standards for classifying a behaviour as abnormal.
General conclusion
None of the above definitions provide a complete definition of abnormality. Mental health (e.g., Jahoda) and mental illness (i.e., the medical model) are probably two-sides of the same coin, but do provide insights of their own. Examining these concepts through statistical deviations from norms does not tell us about the desirability of the deviation. Attempting to define abnormality is in itself a culturally specific task. What seems abnormal in one culture may be seen as perfectly normal in another, and hence it is difficult to define abnormality.
Word count: 2 000
Evaluation of the statistical criterion
The use of statistical frequency and deviation from the statistical norm is not a reliable criterion to define abnormal behaviour since what is ‘abnormal’ in a statistical sense may both be desirable and undesirable. What may be considered abnormal behaviour can differ from one culture to another so it is therefore impossible to establish universal standards for statistical abnormality. The model of statistical deviation from the norm always relates to a specific culture.
Abnormality as deviation from social norms
Social norms constitute informal or formal rules of how individuals are expected to behave. Deviant behaviour is behaviour that is considered undesirable or anti-social by the majority of people in a given society. Individuals who break rules of conduct or do not behave like the majority are defined as ‘abnormal’ according to this criterion.
Social, cultural and historical factors may play a role in what is seen as ‘normal’ or ‘abnormal’ within a certain society. For example, around the 1900s in the UK, homosexuality was seen as abnormal and people could be imprisoned or forcibly treated for this ‘mental illness’. Homosexuality was classified as an abnormal sexual deviation in the DSM-II (1968). In later revisions of the manual, homosexuality in itself was not seen as abnormal – only feeling distressed about it was.
Evaluation of the deviation from statistical norms criterion
This criterion is not objective or stable since it is related to socially based definitions that change across time and culture. Further, because the norm is based on morals and attitudes it is vulnerable to abuse. For example, political dissidents could be considered ‘abnormal’ and sent to hospitals for treatment, which was something that occurred in the former Soviet Union. Using this criterion could lead to discrimination against minorities, including people who suffer from psychological disorders.
Psychological disorders may be defined and diagnosed in different ways across cultures and what seems to be a psychological disorder in one culture may not be seen the same way in another culture. The DSM includes disorders called ‘culture-bound syndromes’; for example, penis panic (!) or Koro. This indicates that it is impossible to set universal standards for classifying a behaviour as abnormal.
General conclusion
None of the above definitions provide a complete definition of abnormality. Mental health (e.g., Jahoda) and mental illness (i.e., the medical model) are probably two-sides of the same coin, but do provide insights of their own. Examining these concepts through statistical deviations from norms does not tell us about the desirability of the deviation. Attempting to define abnormality is in itself a culturally specific task. What seems abnormal in one culture may be seen as perfectly normal in another, and hence it is difficult to define abnormality.
Word count: 2 000
Author: Derek Burton – Passionate about IB Psychology
 RSS Feed
RSS Feed