
IB Psychology students, welcome to the very, very strange world of the placebo.
Our last IB Psychology blog post on nocebos generated a tonne of responses, and also a lot of questions. Some of our IB Psychology students concerned themselves with the fact that while we focused on the nocebo effect, we paid scant attention to the placebo effect ... it was almost as if we were assuming that every student of IB Psychology already had a good in-depth understanding of placebos and the placebo effect. And, to be honest, to some extent we were. The placebo effect is integral to the abnormal option and should feature heavily across multiple IB Psychology learning outcomes, including:
Simply put, a placebo, as defined in IB Psychology, is a substance that has no therapeutic effect, and is used as a control in testing new drugs. However, that simple definition misses so much about the inner workings of the human mind. Placebo ares really, really strange beasts and they throw a whole lot of tricky questions at our knowledge and understanding of the human brain. See the must see video below.
- To what extent do biological, cognitive and sociocultural factors influence abnormal behaviour?
- Evaluate psychological research (that is, theories and/or studies) relevant to the study of abnormal behaviour.
- Examine biomedical, individual and group approaches to treatment.
- Evaluate the use of biomedical, individual and group approaches to the treatment of one disorder.
Simply put, a placebo, as defined in IB Psychology, is a substance that has no therapeutic effect, and is used as a control in testing new drugs. However, that simple definition misses so much about the inner workings of the human mind. Placebo ares really, really strange beasts and they throw a whole lot of tricky questions at our knowledge and understanding of the human brain. See the must see video below.
WELCOME to the STRANGE world of the placebo
Without a doubt, placebos are one of the most interesting and perplexing concepts IB Psychology throws up. The concept also makes for a great IB Psychology Extended Essay, especially when confined a specific concept - such as the efficacy of selective serotonin reuptake inhibitors (SSRIs) in the treatment of depression. However, our focus here is on using the placebo effect in your IB Psychology abnormal option to help you achieve that elusive IB Psychology 7! To that end, here are some key concepts that can be memorised and included in your ERQs:
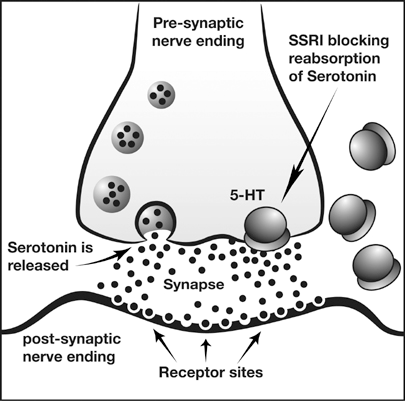
Kirsch et al. (2002) found that there was a publication bias in research into the effectiveness of SSRI in depression. In fact, if the results of all studies (including the ones that had not been published) were pooled together it would seem that the placebo effect accounted for 80% of the antidepressant response. A placebo is a substance that has no therapeutic effect, and is used as a control in testing new drugs. Of the studies funded by pharmaceutical companies, 57% failed to show a statistically significant difference between antidepressant and a neutral placebo. This and similar studies cast doubt on the serotonin hypothesis, not to mention the ethics of drug companies. However, it is still widely promoted by pharmaceutical companies and presumably believed by the 10% of Americans taking these SSRIs to treat depression.
Leauhter et al. (2002) examined changes in brain function during treatment with placebo. The study examined brain function in 51 patients with depression who either received placebo or an active antidepressant medication. An EEG was used to compare brain function in the two experimental groups. The design was double-blind and ran over none weeks. The study used two different SSRI, which were randomly allocated to participants.
Results showed a significant increase in activity in the prefrontal cortex nearly from in the beginning in the trial in the placebo group. The pattern was different from the patients who were treated with the SSRI but patients in both groups got better. This indicates that medication is effective, but placebo is just as effective. The findings from the study are intriguing. The difference in activity in the brain indicates that the brain is perhaps able to heal itself since there was a positive effect for both groups. Believing that they are being treated could be enough for many patients.
These concise and informative key paragraphs above, if reproduced in your IB Psychology exams, will have the examiner ticking all of the knowledge and critical thinking boxes available to her - ensuring you maximum marks!
Remember, we take all of the guess work and all of the hard work out of IB Psychology with our especially prepared model IB Psychology exam answers.
 |  Placebo or real? ... and more importantly, does it even matter?! |
The 60 Minutes segment embedded above provides the IB Psychology student with much insight into the role of placebos in medical research and just how much of the effects of antidepressant medications is probably attributable to the placebo effect (not to mention the pharmaceutical industry exploiting this in highly unethical ways).
Author: Derek Burton – Passionate about IB Psychology







 RSS Feed
RSS Feed