
| The best 5 tips from experienced IB Psychology teachers on how you can achieve that IB Psychology 7. | |
The scary fact is, only four percent of IB Psychology students manage to get a 7 in each examination session. In the video below we show you how to become one of the elite!
How to get a 7 in IB Psychology
Our video above covers these top 5 tips for achieving the IB Psychology 7:
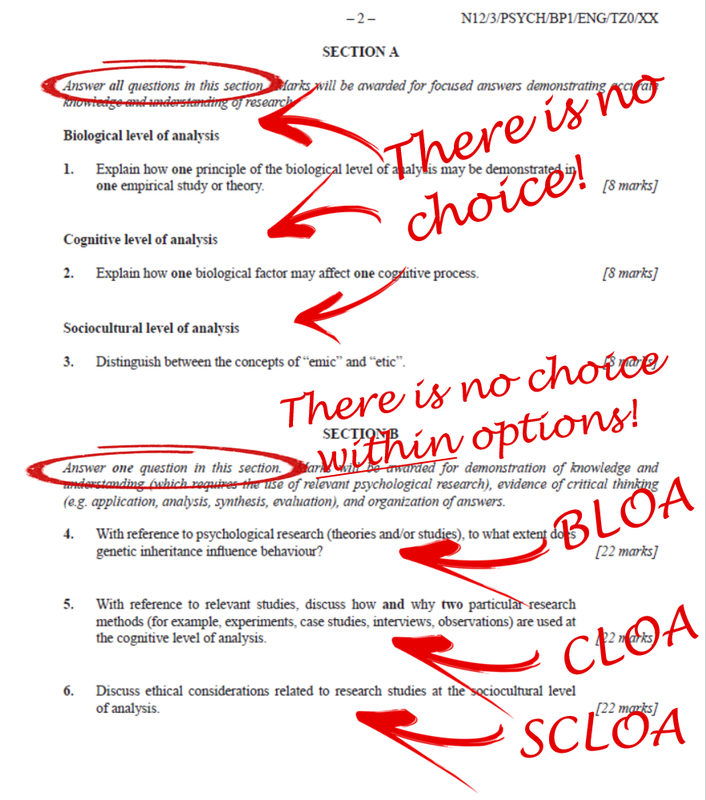
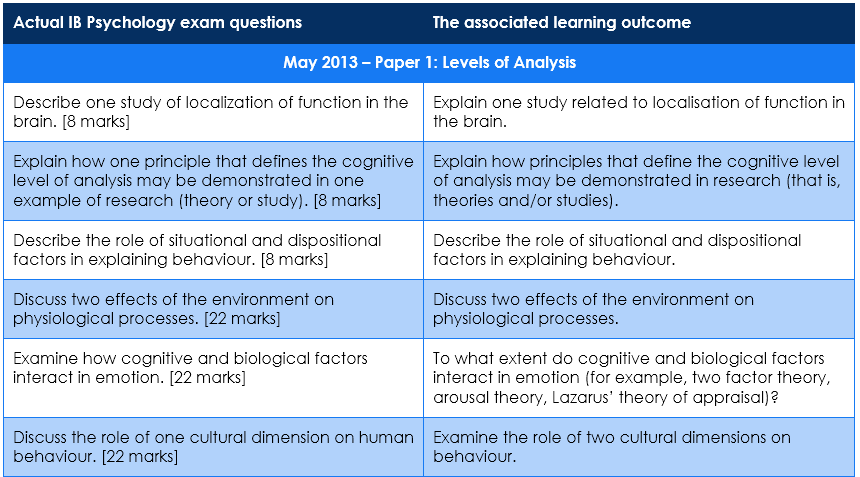
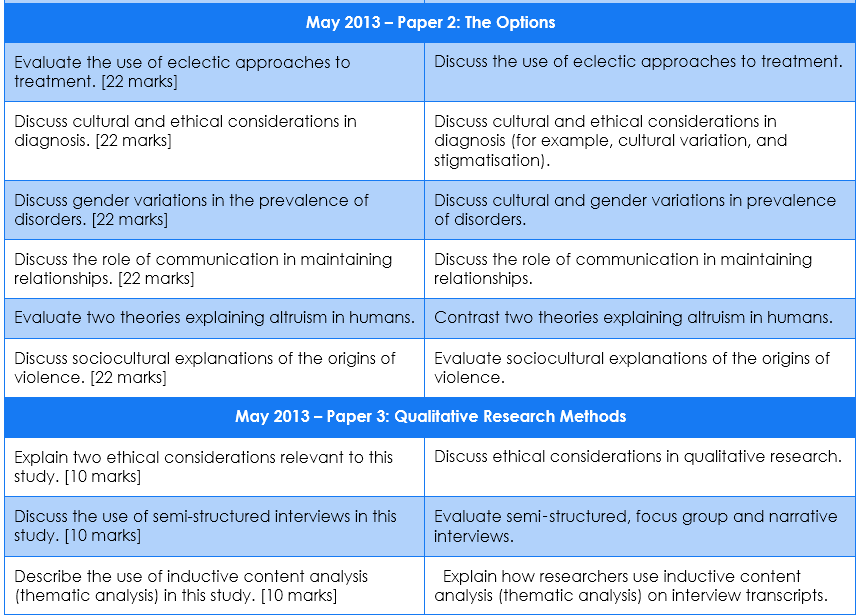
- You already know the questions that can be asked in all 3 of your IB Psychology examination papers! (Yes, really.)
- The IB Psychology Paper 1 examination has three sections - DO NOT study for two of these! (Yes, really.)
- Aim for maximum marks in your IB Psychology IA. (Almost goes without saying.)
- Prepare and memorise model answers to ALL of the extended response questions you are going to target in IB Psychology exams. (But be smart about it!)
- Don’t ignore Qualitative Research Methods, because your IB Psychology teacher almost certainly will! (You need lots of practice with actual stimulus material - i.e., qualitative research)
Author: Derek Burton - Passionate about IB Psychology
 |  |

















 RSS Feed
RSS Feed