
|
We show you exactly what you can get away with when revising for your IB Psychology Paper 2 exams – the Options.
|
|
In the IB Psychology Paper 2 exam – the Options – there is much that you can leave out and still get maximum marks. The Paper 2 exam requires you to answer two extended response question (ERQs) if you are studying Higher Level IB Psychology, and one ERQ if you are studying Standard Level. Each ERQ is worth 22 marks and you should be targeting full marks in this exam. Paper 2 is the easiest exam in which to maximise your overall IB Psychology exam score. It’s the easiest exam for which to prepare model answers to exam questions and then practice these until you can regurgitate them perfectly and “wow!” your IB Psychology examiners.
Take a look at picture below left (click to enlarge). You will see that there are three questions associated with each option, of which you only need to answer one. You will know by now that each question asked in the IB Psychology examinations is straight out of the learning outcomes listed in the IB Psychology Guide (if not, please see one of most popular blog posts here).
Take a look at picture below left (click to enlarge). You will see that there are three questions associated with each option, of which you only need to answer one. You will know by now that each question asked in the IB Psychology examinations is straight out of the learning outcomes listed in the IB Psychology Guide (if not, please see one of most popular blog posts here).
Paper 2 exam questions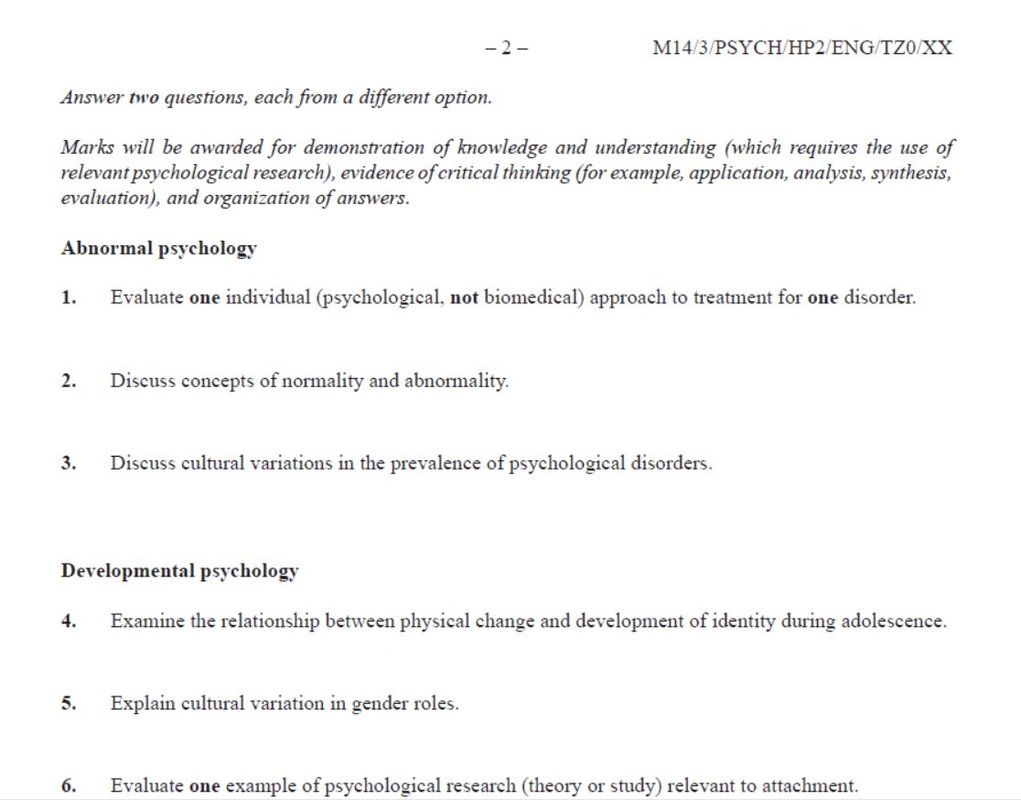
Remember, the IB Psychology LOs listed in the Guide, are your actual exam questions.
|
Abnormal Learning outcomes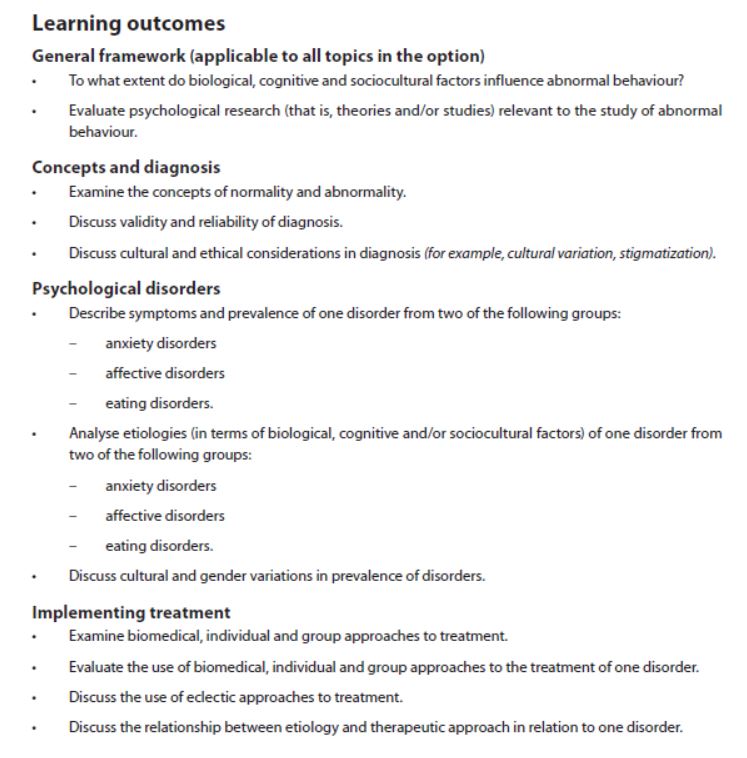
|
Now if you have a look above right (click to enlarge), at the learning outcomes associated with one of the IB Psychology options – Abnormal Psychology, you might think that there is quite a bit of preparation and revision that you need to do. 12 learning outcomes would equate to preparing and memorising 12 model answers, just for this one option, right? Wrong! Let me explain …
Firstly, within each option you have three essay question (ERQ) choices. Secondly, there has never been, nor is there likely to ever be, an IB Psychology exam where all three questions come from within a single subsection such as “Concepts and Diagnosis” or “Psychological Disorders” in the Abnormal option. This means that you can eliminate one ERQ from each of these sections. Thirdly, IB Psychology examiners can’t set an ERQ exam question based on a lower level command terms such as “explain”, “analyse” or “describe”. Very occasionally you will see exam question twisted and contorted to mix a lower level question term and a higher level command term. It hardly ever happens, you have other questions to choose from, so go ahead, cross these LOs off your list too.
Take a look below (again, click to enlarge) at how many Human Relationship LOs you will need to prepare model answers and revise for if you follow this advice. Instead of revising for 13 LOs, you now only need prepare and revise for six! And because you are now only focussing on six ERQ questions, you can prepare perfect 22/22 answers, commit them to memory and regurgitate them as soon as the IB Psychology Paper 2 exam begins. Genius! (At least your IB Psychology examiner will think you are!)
Firstly, within each option you have three essay question (ERQ) choices. Secondly, there has never been, nor is there likely to ever be, an IB Psychology exam where all three questions come from within a single subsection such as “Concepts and Diagnosis” or “Psychological Disorders” in the Abnormal option. This means that you can eliminate one ERQ from each of these sections. Thirdly, IB Psychology examiners can’t set an ERQ exam question based on a lower level command terms such as “explain”, “analyse” or “describe”. Very occasionally you will see exam question twisted and contorted to mix a lower level question term and a higher level command term. It hardly ever happens, you have other questions to choose from, so go ahead, cross these LOs off your list too.
Take a look below (again, click to enlarge) at how many Human Relationship LOs you will need to prepare model answers and revise for if you follow this advice. Instead of revising for 13 LOs, you now only need prepare and revise for six! And because you are now only focussing on six ERQ questions, you can prepare perfect 22/22 answers, commit them to memory and regurgitate them as soon as the IB Psychology Paper 2 exam begins. Genius! (At least your IB Psychology examiner will think you are!)
FRom 13 → 6 Learning Outcomes!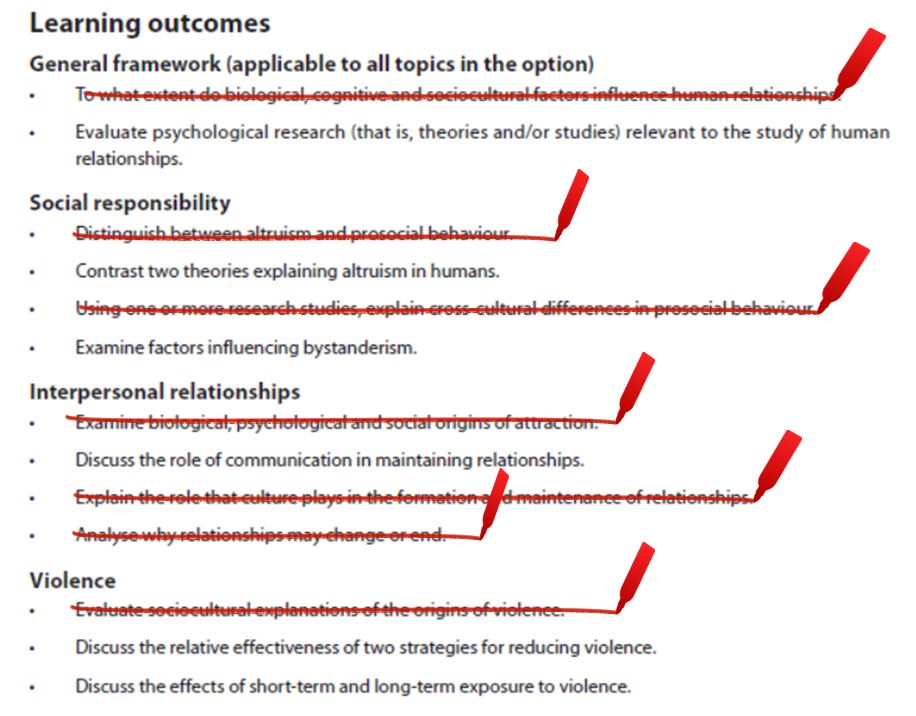
|
|

|
|
Remember, wwwPsychologyIB.com has model ERQ answers for the two most popular IB Psychology options – Abnormal and Human Relationships, and we guarantee you will be awarded 22/22 marks if you can replicate them in your exams.
Author: Derek Burton - Passionate about IB Psychology

















 RSS Feed
RSS Feed